Related Articles



Key Takeaways for Severe Toenail Fungus Treatment: Lamisil vs Sporanox Comparison
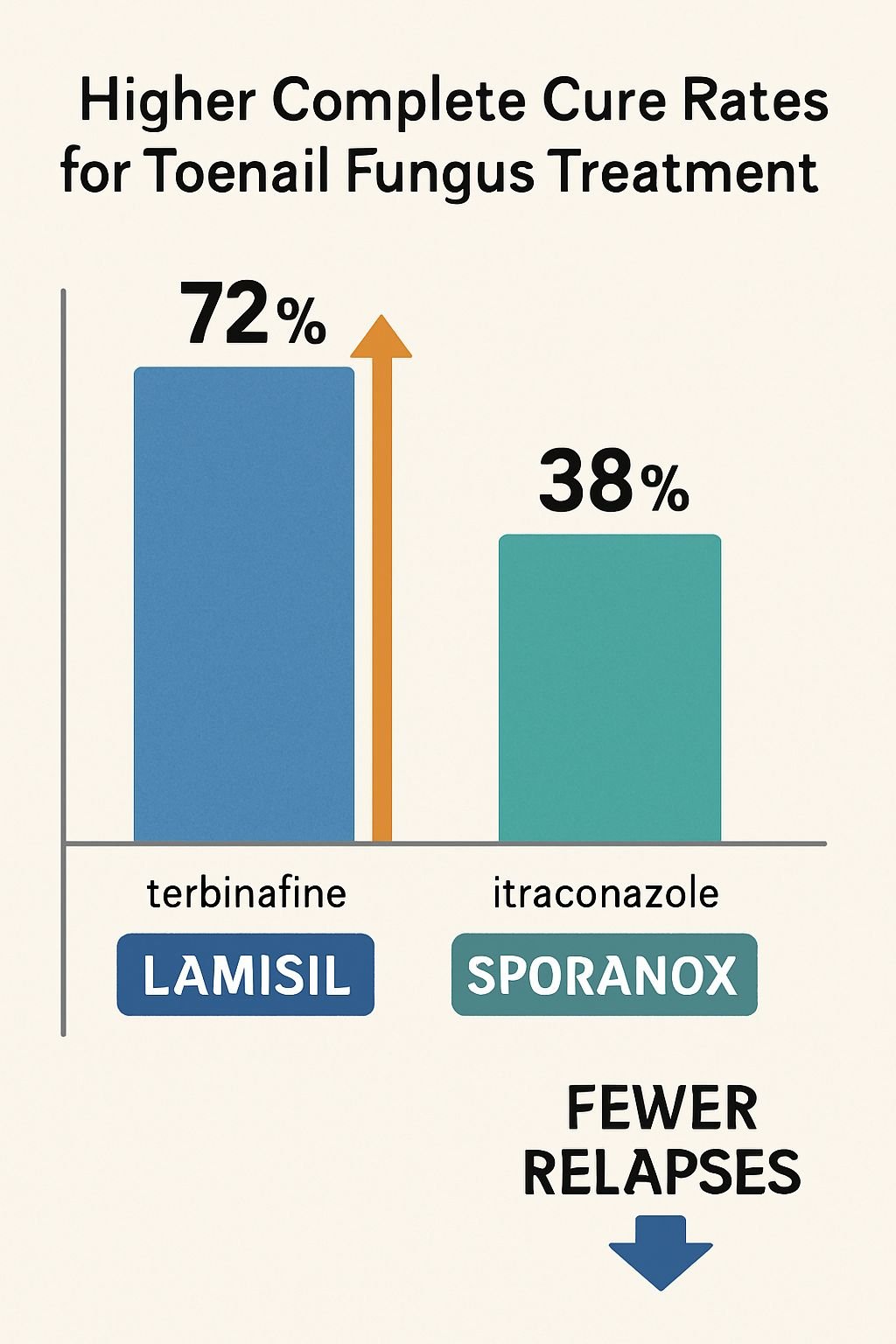
- Lamisil (terbinafine) demonstrates higher complete cure rates than Sporanox (itraconazole) for toenail fungus treatment, with fewer relapses after treatment completion.
- Prescription oral antifungals are necessary for severe toenail fungus as they target the infection systemically, unlike topical treatments that can’t penetrate deeply enough to reach the nail bed.
- Lamisil works by inhibiting squalene epoxidase in fungal cells, while Sporanox disrupts ergosterol production – both mechanisms effectively kill the fungus rather than just preventing growth.
- Treatment duration typically ranges from 6-12 weeks for oral medications, though visible improvement may take months as healthy nail needs time to grow out completely.
- Both medications require liver function testing before and during treatment, and each has unique drug interactions that must be carefully evaluated by your healthcare provider.
Toenail fungus might seem like just a cosmetic issue, but when it becomes severe, it requires serious medical intervention. Finding the right treatment makes all the difference between recurring infections and complete healing.
If you’re battling stubborn toenail fungus, you’ve likely encountered recommendations for prescription medications like Lamisil and Sporanox. These powerful antifungals represent the gold standard in treatment for severe cases, with clinical studies showing significantly higher success rates compared to over-the-counter options. But how do you know which one might work better for your specific situation?
In this comprehensive comparison, we’ll examine the effectiveness, safety profiles, and practical considerations for both medications to help you have an informed conversation with your healthcare provider about your best treatment path forward.

Why Severe Toenail Fungus Requires Prescription Treatment
Toenail fungus, medically known as onychomycosis, can progress from a minor discoloration to a serious infection that causes nail thickening, brittleness, and even separation from the nail bed. While many people attempt to address early infections with topical solutions, these treatments often fail to penetrate deeply enough to reach the fungus embedded beneath the nail.
Prescription oral antifungals become necessary when the infection penetrates the nail matrix or when significant portions of the nail are affected. The fungi responsible for these infections burrow deep into the nail bed where topical treatments simply cannot reach. This explains why approximately 35-50% of nail fungus cases don’t respond to topical treatments alone.
Additionally, certain risk factors such as diabetes, circulatory problems, or compromised immune systems can make fungal infections particularly resistant and potentially dangerous. In these cases, oral medications like Lamisil and Sporanox are typically prescribed to attack the infection systemically through the bloodstream, delivering the medication directly to the infected nail bed.
How Lamisil Works Against Stubborn Toenail Fungus
Lamisil, containing the active ingredient terbinafine, works differently than many other antifungal medications. Rather than simply slowing fungal growth, it actually kills the fungus by disrupting a critical component of the fungal cell membrane formation process. This fungicidal (versus fungistatic) action is one reason for its impressive effectiveness. For more information on effective treatments, check out our guide on the best prescription treatments for toenail fungus.
The medication circulates through your bloodstream and concentrates in the nail bed, where it actively attacks the fungal infection. Importantly, Lamisil remains in the nail tissue for months after you’ve stopped taking the medication, providing continued protection against recurrence.
- Targets squalene epoxidase, preventing ergosterol synthesis
- Creates fungal cell membrane defects, leading to cell death
- Concentrates in keratin-rich tissues like nails
- Persists in nail tissue for 3-6 months after treatment ends
- Shows effectiveness against dermatophytes, the most common cause of nail fungus
Active Ingredient Terbinafine’s Mechanism of Action
Terbinafine’s effectiveness stems from its unique mechanism of action. Unlike azole antifungals that target a later stage in the ergosterol synthesis pathway, terbinafine inhibits squalene epoxidase, an enzyme crucial for fungal cell membrane integrity. This interference creates a buildup of squalene within the fungal cell while simultaneously depleting ergosterol, a vital component of fungal cell membranes.
This dual action leads to increased cell permeability and ultimately results in fungal cell death. The specificity of terbinafine for fungal enzymes over mammalian ones contributes to its favorable safety profile compared to some alternative treatments. Additionally, its lipophilic nature allows it to distribute effectively into the nail matrix, nail bed, and nail plate, where the infection resides.
Typical Dosage and Treatment Duration
The standard Lamisil treatment protocol for toenail fungus consists of 250mg tablets taken once daily for 12 weeks. This regimen has been established through extensive clinical trials as the optimal duration to achieve maximum cure rates while minimizing side effects. For more information on effective approaches, you can explore severe to mild toenail fungus treatments.
Standard Lamisil Treatment for Toenail Fungus
Dosage: 250mg tablet
Frequency: Once daily
Duration: 12 weeks (3 months)
Administration: Can be taken with or without food
Liver function monitoring: Before treatment and at 4-6 weeks
While the medication is typically taken for 12 weeks, the visible improvement continues long after treatment concludes. Complete clearing of the infection requires the healthy nail to grow out fully, which can take 9-12 months for toenails. Patients should understand this timeline to maintain realistic expectations about when they’ll see full results.
Success Rates in Clinical Studies
Clinical trials consistently demonstrate Lamisil’s superior efficacy in treating onychomycosis compared to many alternatives. In head-to-head studies, terbinafine has shown complete cure rates of 38-76%, depending on severity and duration of the infection before treatment began. These numbers significantly outperform both placebo treatments and many competing antifungals.
Long-term follow-up studies also reveal that Lamisil maintains its effectiveness with relatively low recurrence rates. In a notable 5-year follow-up study, approximately 21% of successfully treated patients experienced recurrence, compared to higher rates with other treatments. This sustained effectiveness is attributed to terbinafine’s fungicidal action and its persistence in nail tissue long after the treatment course ends.
The medication proves particularly effective against dermatophytes like Trichophyton rubrum, the most common cause of toenail fungus. However, it shows somewhat lower efficacy against certain yeast infections, which becomes an important consideration when determining the appropriate treatment for specific fungal types.
How Sporanox Tackles Severe Fungal Infections
Sporanox (itraconazole) approaches fungal infections through a different biochemical pathway than Lamisil. This broad-spectrum antifungal belongs to the triazole class of medications that work by inhibiting the fungal enzyme 14-alpha-demethylase, which is necessary for converting lanosterol to ergosterol, an essential component of fungal cell membranes.
By disrupting ergosterol production, Sporanox weakens the fungal cell membrane, causing increased permeability that leads to leakage of cellular contents and ultimately fungal death. This mechanism makes Sporanox effective against a wider variety of fungal species than some other antifungals, including certain yeasts and molds that might not respond as well to Lamisil.
Sporanox also has the advantage of treating fungal infections beyond just the nails, making it valuable for patients with multiple fungal infection sites. Its versatility in treating both dermatophytes and certain non-dermatophyte molds expands its utility in complex cases where multiple fungal species might be present. For more information on effective treatments, check out our guide on the best prescription treatments for toenail fungus.
Itraconazole’s Method of Fighting Fungus
Itraconazole functions by binding to fungal cytochrome P450 enzymes, specifically 14-alpha-demethylase. This enzyme inhibition prevents the conversion of lanosterol to ergosterol, causing an accumulation of 14-alpha-methylsterols. Without sufficient ergosterol, fungal cells cannot maintain proper membrane integrity and function. For a detailed comparison of antifungal treatments, check out the Lamisil vs Sporanox comparison.
Unlike some antifungals that merely prevent fungal growth, itraconazole’s action can be fungicidal at sufficient concentrations. The medication demonstrates high affinity for keratinized tissues like nails, which contributes to its effectiveness in treating onychomycosis. Additionally, Sporanox reaches therapeutic concentrations in the nail plate within two weeks of starting therapy and can remain detectable in nail clippings for up to six months after discontinuation.
Pulse Therapy vs. Continuous Treatment Options
One of Sporanox’s unique features is the option for pulse therapy rather than continuous daily dosing. Standard continuous therapy involves taking 200mg of itraconazole daily for 12 weeks for toenail fungus. Pulse therapy, by contrast, consists of taking 200mg twice daily for one week per month, repeated for 3-4 months.
|
Treatment Approach |
Dosage |
Schedule |
Total Duration |
|---|---|---|---|
|
Continuous Therapy |
200mg once daily |
Every day |
12 weeks |
|
Pulse Therapy |
200mg twice daily |
1 week on, 3 weeks off |
3-4 months |
Pulse therapy offers several advantages, including potentially better compliance, reduced cost, and fewer side effects while still maintaining therapeutic levels in the nail tissue. Studies indicate comparable efficacy between pulse and continuous therapy for many patients, though continuous therapy might be preferred for more severe or resistant infections.
Documented Effectiveness for Different Fungal Types
Sporanox demonstrates broader antifungal activity than many competitors, making it particularly valuable for infections caused by non-dermatophyte molds or yeasts that might not respond as well to terbinafine. Clinical studies show complete cure rates of 25-40% for toenail fungus after a standard treatment course, which is somewhat lower than Lamisil but still significantly better than placebo or topical treatments alone.
The medication shows particularly strong effectiveness against Candida species, certain Aspergillus infections, and dimorphic fungi that Lamisil might not adequately address. This spectrum of activity makes Sporanox a valuable option for patients with mixed infections or those who have failed previous treatment with terbinafine.
However, the mycological cure rates (elimination of fungus on laboratory testing) tend to be higher than complete cure rates (both mycological cure and normal nail appearance), suggesting that while Sporanox effectively kills the fungus, full nail restoration may take longer or remain incomplete in some patients.
Head-to-Head Effectiveness Comparison
When directly compared in clinical trials, Lamisil consistently outperforms Sporanox in treating dermatophyte onychomycosis, which accounts for approximately 90% of toenail fungus cases. A landmark double-blind study found that after 12 weeks of treatment, Lamisil produced complete cure rates of 76% compared to Sporanox’s 38%, a statistically significant difference.
However, the picture becomes more nuanced when examining specific fungal species. For dermatophytes like Trichophyton rubrum and T. mentagrophytes, Lamisil maintains its superior position. But for Candida infections and certain non-dermatophyte molds, Sporanox may provide better results in some cases. This highlights the importance of proper fungal identification through laboratory testing before selecting a treatment approach.
Clinical Trial Results: Which Medication Clears Infections Faster?
Time to improvement represents a critical factor for patients suffering from uncomfortable or unsightly nail fungus. Clinical evidence indicates that both medications begin working within weeks, though visible results take longer due to the slow growth rate of nails. Lamisil typically shows faster initial clearance, with patients noticing improvement in nail appearance at 4-6 weeks compared to 6-8 weeks with Sporanox.
Recurrence Rates After Treatment
Long-term studies reveal significant differences in recurrence rates between the two medications. Patients treated with Lamisil experience recurrence in approximately 15-20% of cases within five years of completing therapy. In contrast, Sporanox has shown higher recurrence rates of 25-30% within the same timeframe.
This difference in relapse rates likely stems from Lamisil’s fungicidal action and its longer persistence in nail tissue after treatment ends. Terbinafine remains active in nail keratin for up to 6 months after discontinuation, providing extended protection as the healthy nail grows out. Itraconazole, while also detectable in nail tissue after treatment ends, typically persists for a shorter duration and at lower concentrations.
Visible Improvement Timelines
Patients understandably want to know when they’ll see results. With both medications, visible improvement follows a predictable timeline, though complete clearing requires patience. Initial signs of improvement typically appear within 4-8 weeks as new, healthy nail begins growing from the base. However, complete clearing depends on the growth rate of toenails, which advances approximately 1mm per month.
For typical toenail fungus affecting the entire nail, complete visual clearing may take 9-12 months regardless of which medication is chosen. Patients should understand this timeline to maintain realistic expectations. Lamisil tends to show visible improvement slightly faster in most cases, with clinical studies documenting higher rates of partial clearing at 3-month assessment points.
Documentation with periodic photographs is recommended to track progress objectively, as day-to-day observation may make improvements difficult to perceive.
Side Effect Profiles: What to Expect
Both medications carry risks of side effects, though most patients tolerate treatment well. Understanding potential adverse reactions helps patients recognize issues that warrant medical attention versus minor effects that typically resolve on their own. For a detailed comparison of these treatments, you can visit this Lamisil vs Sporanox guide.
Overall safety profiles for both medications are well-established through decades of clinical use. However, significant differences exist in their side effect patterns and monitoring requirements that can influence medication selection based on individual health factors.
Common Lamisil Side Effects and Their Frequency
Lamisil’s most frequent side effects tend to be mild and gastrointestinal in nature. Approximately 5-15% of patients experience symptoms like mild stomach upset, diarrhea, or altered taste sensation. For more information on Lamisil vs Sporanox, these symptoms rarely require discontinuation of therapy and often improve as treatment continues.
Skin reactions occur in about 2% of patients and can include rash, itching, or hives. More serious but rare dermatological reactions like Stevens-Johnson syndrome have been reported in fewer than 0.01% of cases. Elevated liver enzymes without symptoms occur in approximately 3-5% of patients, which is why liver function testing is recommended before and during treatment.
- Headache (12-13% of patients)
- Gastrointestinal disturbances (5-15%)
- Taste disturbance (2-3%)
- Rash or itching (2%)
- Elevated liver enzymes without symptoms (3-5%)
- Serious liver reactions (rare, <0.1%)
Typical Sporanox Adverse Reactions
Sporanox demonstrates a somewhat different side effect profile than Lamisil. Gastrointestinal effects remain common, with nausea affecting approximately 10% of patients and abdominal discomfort reported in 5-8% of cases. Headache occurs in roughly 10% of those taking the medication. For more information on effective treatments, you can explore prescription treatments for toenail fungus.
One significant difference is Sporanox’s potential for cardiovascular effects. The medication can cause QT interval prolongation in some patients, which increases the risk of serious cardiac arrhythmias. This risk is substantially higher in patients with existing heart conditions or those taking certain other medications. Additionally, Sporanox demonstrates more extensive drug interactions than Lamisil, requiring careful medication review before initiation. For more information on treatments, you can explore prescription treatments for toenail fungus.
Elevated liver enzymes occur at similar rates to Lamisil, affecting approximately 4% of patients. However, the risk of symptomatic hepatitis appears slightly higher with Sporanox based on post-marketing surveillance data.
Serious Side Effect Risks with Both Medications
Though rare, both medications can cause serious adverse reactions that require immediate medical attention. Liver toxicity represents the most significant concern for both drugs, with symptoms including jaundice (yellowing of skin/eyes), dark urine, pale stools, unusual fatigue, or abdominal pain. These symptoms warrant immediate discontinuation and medical evaluation.
Serious skin reactions including Stevens-Johnson syndrome or toxic epidermal necrolysis occur in fewer than 1 in 10,000 patients but require emergency care if they develop. Signs include widespread rash, blistering, or peeling skin, especially if accompanied by fever, sore throat, or mucosal involvement.
When to Seek Emergency Care During Treatment
• Yellowing of skin or eyes
• Unusual fatigue or weakness
• Dark urine or pale stools
• Upper right abdominal pain
• Widespread rash, especially with blistering
• Difficulty breathing or swallowing
• Irregular heartbeat (particularly with Sporanox)
Both medications can also rarely cause blood disorders, neurological effects, or allergic reactions. The overall incidence of serious adverse events remains below 1% with proper patient selection and monitoring.
Who Should Avoid Each Medication
Certain medical conditions create absolute or relative contraindications for these medications. Lamisil should be avoided in patients with active or chronic liver disease, severe renal impairment (creatinine clearance <50 mL/min), or known hypersensitivity to terbinafine compounds. Caution is advised in patients with autoimmune conditions due to rare reports of lupus-like syndromes.
Sporanox has more extensive contraindications, including pregnancy, heart failure, ventricular dysfunction, and history of heart rhythm disorders. It should not be used concomitantly with numerous medications including certain statins, sedatives, and anti-arrhythmics due to potentially dangerous interactions. Patients with hypochlorhydria or achlorhydria (low stomach acid) may have reduced absorption of itraconazole capsules.
Both medications warrant caution in elderly patients, who may experience more significant side effects or drug interactions due to age-related changes in metabolism and elimination. Careful consideration of benefit-to-risk ratio becomes particularly important in these populations.
Drug Interaction Concerns
Managing potential drug interactions represents a critical aspect of treatment selection. Both Lamisil and Sporanox can interact with other medications, though Sporanox demonstrates significantly more extensive interaction potential due to its effects on hepatic cytochrome enzymes.
A thorough medication review must be conducted before starting either treatment to prevent potentially dangerous combinations. This review should include prescription medications, over-the-counter drugs, supplements, and herbal remedies.
Medications That Conflict with Lamisil
Lamisil has relatively few significant drug interactions compared to many antifungals. It moderately inhibits CYP2D6 enzymes, potentially increasing blood levels of medications metabolized through this pathway. Drugs with narrow therapeutic windows that use this pathway include certain antidepressants, antipsychotics, beta-blockers, and class 1C antiarrhythmics.
Caffeine clearance may be reduced by approximately 20% in patients taking Lamisil, potentially increasing caffeine effects. Cimetidine can increase terbinafine blood levels by about 30%, potentially increasing side effect risk. Rifampin may reduce terbinafine levels by approximately 40%, potentially reducing effectiveness.
- Selective serotonin reuptake inhibitors (SSRIs)
- Tricyclic antidepressants
- Beta-blockers (particularly metoprolol)
- Dextromethorphan (in some cough medications)
- Certain antiarrhythmics (flecainide, propafenone)
Sporanox’s Extensive Interaction List
Sporanox presents substantially more complex interaction concerns through its strong inhibition of CYP3A4 enzymes. This enzyme system metabolizes approximately 50% of commonly prescribed medications, creating numerous potential interactions. Concurrent use with certain medications is absolutely contraindicated due to risk of serious cardiac arrhythmias, rhabdomyolysis, or respiratory depression.
The FDA has issued specific warnings against combining Sporanox with several medications including cisapride, pimozide, quinidine, dofetilide, triazolam, oral midazolam, certain statins, and ergot alkaloids. These combinations have been associated with life-threatening adverse events. Additionally, medications that induce CYP3A4 can dramatically reduce Sporanox effectiveness, potentially leading to treatment failure.
Acid-reducing medications like proton pump inhibitors and H2 blockers significantly reduce Sporanox absorption, potentially rendering treatment ineffective. Patients requiring these medications may need alternative antifungal therapy or special administration instructions.
Impact on Heart Medications and Other Critical Drugs
Cardiac patients face particular challenges with antifungal selection. Sporanox can increase levels of many cardiac medications to potentially dangerous levels, including calcium channel blockers, digoxin, and certain antiarrhythmics. Additionally, it can prolong the QT interval independently, further increasing arrhythmia risk when combined with other QT-prolonging medications.
Patients taking warfarin or similar anticoagulants may experience altered anticoagulant effects with either medication, though the interaction is more significant with Sporanox. More frequent INR monitoring is recommended during treatment initiation and after discontinuation. Diabetic patients taking oral hypoglycemics generally have minimal interaction concerns with Lamisil, while Sporanox may affect blood levels of certain diabetes medications.
|
Medication Category |
Interaction with Lamisil |
Interaction with Sporanox |
|---|---|---|
|
Statins |
Minimal |
Major – contraindicated with some |
|
Calcium Channel Blockers |
Minimal |
Significant – dose adjustment needed |
|
Warfarin |
Minor |
Moderate – monitoring required |
|
Benzodiazepines |
Minimal |
Major – some contraindicated |
|
Oral Contraceptives |
None reported |
Minimal |
Cost Comparison and Insurance Coverage
Treatment affordability represents a significant consideration for many patients. Generic forms of both medications have substantially reduced costs compared to their brand-name counterparts, though meaningful price differences remain between the treatment options.
As of current pricing data, generic terbinafine typically costs approximately $30-60 for a complete 12-week treatment course. Generic itraconazole generally ranges from $80-150 for a similar treatment duration using continuous therapy, or approximately $100-180 for pulse therapy. Brand name versions cost substantially more, with Lamisil averaging $500-700 and Sporanox $800-1,200 for complete treatment courses.
Average Pricing for Complete Treatment Courses
The total cost of treatment extends beyond just medication prices. Both medications require baseline liver function testing before treatment initiation, adding approximately $50-150 depending on laboratory and insurance coverage. Lamisil typically requires one follow-up liver panel at 6 weeks, while continuous Sporanox therapy may warrant monthly monitoring, potentially adding $100-300 to the total treatment cost.
When calculating overall treatment expense, patients should consider potential hidden costs like follow-up appointments, additional testing, and possible management of side effects. The lower likelihood of treatment failure with Lamisil in typical dermatophyte infections may represent additional cost savings by reducing the need for secondary treatments.
Estimated Total Treatment Costs
Generic terbinafine (Lamisil): $80-210
• Medication: $30-60
• Laboratory tests: $50-150Generic itraconazole (Sporanox): $180-450
• Medication: $80-150
• Laboratory tests: $100-300
Generic vs. Brand Name Options
Generic formulations have substantially improved affordability for both medications. Terbinafine became available as a generic in 2007, while itraconazole followed in 2010. These generic options contain the same active ingredients at identical dosages, but may use different inactive ingredients (fillers, binders, coatings) that rarely affect treatment outcomes.
Bioequivalence studies confirm that generic versions deliver the same amount of medication to the bloodstream within the same timeframe as their brand-name counterparts. Quality concerns that existed with early generic formulations have largely been addressed through improved manufacturing processes and regulatory oversight. For most patients, generic options provide equivalent therapeutic benefits at a fraction of the cost.
In rare cases, patients may experience different side effects with generic formulations due to inactive ingredients. If this occurs, discussing specific manufacturer preferences with your pharmacist may help identify a better-tolerated alternative while still maintaining cost savings.
Typical Insurance Coverage Limitations
Insurance coverage for antifungal medications varies widely between plans. Many insurance providers require prior authorization for these medications, requiring documentation of positive fungal culture or other confirmation of infection. Some plans limit coverage to patients with specific risk factors like diabetes or immunosuppression, considering treatment “cosmetic” for other individuals.
When coverage is approved, most plans place these medications in Tier 2 or Tier 3 categories, with copays ranging from $30-75 per fill. Medicare Part D plans typically cover generic versions with similar copay structures, though coverage gaps may create temporary periods of higher out-of-pocket costs. Manufacturer assistance programs exist for brand-name versions but rarely for generics. For more information on effective treatments, explore effective approaches to toenail fungus treatment.
Which Medication Is Right for You?
Selecting the optimal treatment requires balancing effectiveness, safety, cost, and individual factors. While general recommendations can be made based on infection characteristics, final decisions should incorporate patient-specific considerations including medical history, concurrent medications, and personal preferences. For more information on prescription treatments for toenail fungus, explore our detailed guide.
For most uncomplicated dermatophyte infections affecting the toenails, Lamisil typically represents the first-line choice due to its higher cure rates, fewer drug interactions, and typically lower cost. However, several scenarios may warrant consideration of Sporanox as an alternative or preferred option.
Best Choice for Diabetic Patients
Diabetic patients face particular challenges with fungal nail infections. Reduced circulation, altered immune response, and elevated glucose levels create an environment that favors fungal growth while reducing treatment effectiveness. Additionally, these infections pose greater risks for diabetic patients, potentially creating entry points for secondary bacterial infections.
For most diabetic patients with confirmed dermatophyte infections, Lamisil remains the first-line treatment due to its superior effectiveness. Its minimal interaction with common diabetes medications also simplifies treatment. However, patients with diabetic nephropathy (kidney damage) may require dosage adjustments or alternative treatments if renal function is significantly impaired.
Close monitoring of blood glucose becomes particularly important during treatment, as some patients report mild fluctuations with both medications. Diabetic patients should also receive education about proper foot care during and after treatment to reduce recurrence risk.
- Monitor blood glucose more frequently during first 2 weeks of treatment
- Inspect feet daily for any new lesions or signs of secondary infection
- Maintain excellent glycemic control to improve treatment outcomes
- Consider prophylactic topical antifungals after successful treatment
- Discuss comprehensive diabetic foot care with your provider
Recommendations for Patients with Heart or Liver Conditions
Heart conditions significantly influence medication selection. Sporanox is generally contraindicated in patients with ventricular dysfunction, heart failure, or history of ventricular arrhythmias due to its potential to prolong the QT interval and interact with cardiac medications. For these patients, Lamisil typically represents the safer option, though baseline ECG testing may be recommended for older adults or those with multiple cardiac risk factors.
Liver concerns create considerations with both medications. All patients should undergo baseline liver function testing before starting either treatment. Those with mild abnormalities in liver enzymes may still safely use these medications with more frequent monitoring, but patients with active liver disease or cirrhosis should generally avoid both options. For a detailed comparison of these treatments, you can refer to this Lamisil vs Sporanox guide.
Antifungal Recommendations Based on Medical Conditions
Congestive Heart Failure: Lamisil preferred, Sporanox contraindicated
Ventricular Arrhythmias: Lamisil preferred, Sporanox contraindicated
Stable Coronary Artery Disease: Either medication with proper monitoring
Mild Hepatic Impairment: Either medication with increased monitoring
Moderate-Severe Hepatic Impairment: Both medications typically avoided
Renal Impairment: Adjusted Lamisil dosing or Sporanox pulse therapy
For patients with both cardiac and hepatic concerns, topical treatments or mechanical debridement may represent more appropriate management strategies despite their lower effectiveness. The risk-benefit calculation shifts substantially when multiple organ systems face potential medication effects.
Consultation with specialists may be warranted before initiating treatment in complex cases, particularly when patients have multiple comorbidities or take several medications with potential interactions.
When Your Doctor Might Choose One Over the Other
Several clinical scenarios may influence your doctor’s recommendation beyond basic effectiveness considerations. If laboratory testing identifies non-dermatophyte molds or certain yeast species as the causative organisms, Sporanox may offer superior activity despite its generally lower cure rates for typical dermatophyte infections. This highlights the value of proper fungal identification before treatment initiation when possible.
Patients with a history of inflammatory bowel disease sometimes tolerate Sporanox better than Lamisil, as the latter has been associated with rare exacerbations of these conditions. Conversely, patients taking multiple medications generally experience fewer interaction concerns with Lamisil, making it preferable in complex medication regimens.
Treatment history also influences selection. Patients who previously failed treatment with one agent might benefit from switching to the alternative. Those who experienced side effects with one medication but still require systemic therapy might tolerate the other option better due to different side effect profiles.
- Non-dermatophyte infection: Sporanox often preferred
- Multiple concurrent medications: Lamisil typically preferred
- Previous terbinafine failure: Sporanox offers alternative mechanism
- Inflammatory bowel disease: Sporanox may be better tolerated
- Compliance concerns: Sporanox pulse therapy might improve adherence
What to Do If First-Line Treatment Fails
Despite optimal treatment, approximately 20-30% of patients experience inadequate response to their initial antifungal therapy. When this occurs, several strategies may be employed. The first step involves confirming continued presence of infection through follow-up cultures or microscopic examination, as apparent treatment failure sometimes represents other nail conditions like psoriasis or trauma. If infection persists, switching to the alternative oral antifungal often produces success, particularly if the initial treatment targeted the wrong fungal type. Combination approaches using both oral and topical medications simultaneously may provide synergistic benefits in resistant cases. For truly refractory infections, nail removal (permanent or temporary) combined with antifungal therapy offers the highest cure rates but represents a more aggressive approach reserved for severe cases.
Frequently Asked Questions
Patients commonly have questions about these treatments that extend beyond basic effectiveness comparisons. Understanding practical aspects of treatment helps set appropriate expectations and improves compliance. The following addresses the most frequent inquiries about these medications.
Remember that while this information provides general guidance, individual circumstances may require personalized recommendations from your healthcare provider.
How long will I need to take Lamisil or Sporanox to see results?
Both medications require patience before visible improvements appear. Initial signs of success typically emerge within 6-8 weeks as new, healthy nail begins growing from the base. However, complete clearing depends on the growth rate of your toenails, which advances approximately 1mm per month on average. For more information on effective treatments, you can explore rapid toenail fungus treatment options.
Typical Timeline for Visible Improvement
Weeks 1-4: No visible change in nail appearance
Weeks 6-8: Clear nail beginning to grow from base
Months 3-6: Partial clearing as healthy nail advances
Months 9-12: Complete replacement of infected nail
(Timeline varies based on individual growth rates and infection severity)The medication itself remains active in your nail tissue for months after you stop taking it. Lamisil can be detected in nail clippings for up to 6 months after completing therapy, while Sporanox typically persists for 3-4 months. This extended presence continues fighting the infection as your nail grows out. For more information on effective treatments, explore severe and mild toenail fungus treatment approaches.
Taking photos of your nails monthly can help document progress objectively. Daily observation makes improvements difficult to notice, while periodic documentation allows you to see gradual changes more clearly.
If you see no improvement whatsoever after 3 months of treatment, consult your doctor. This may indicate misdiagnosis, resistant infection, or need for alternative approaches.
Can I drink alcohol while taking either medication?
Moderate alcohol consumption (1-2 drinks occasionally) generally doesn’t significantly impact treatment with either medication. However, both drugs undergo liver metabolism, and alcohol places additional demands on liver function. Heavy or daily drinking should be avoided during treatment with either medication to reduce liver stress and potential for hepatotoxicity. For more information, you can compare Lamisil vs Sporanox to understand their effects.
Sporanox demonstrates somewhat greater concerns with alcohol interaction due to its more extensive liver metabolism and higher baseline liver enzyme elevation rates. If you choose to drink while taking these medications, staying well below recommended weekly limits (7 drinks for women, 14 for men) and avoiding daily consumption represents the safest approach.
Will my insurance cover these prescription antifungal medications?
Most insurance plans cover these medications when medical necessity is documented, though coverage details vary significantly between plans. Many insurers require confirmation of infection through positive culture or microscopic examination rather than visual diagnosis alone. Some plans limit coverage to patients with risk factors like diabetes or require documentation of failed topical treatments before approving oral options. When approved, typical copays range from $10-60 for generics depending on your specific plan design. Medicare Part D plans generally cover generic versions of both medications with similar requirements.
If coverage is denied, patient assistance programs exist for brand-name versions, while discount programs like GoodRx can substantially reduce out-of-pocket costs for generics. Generic terbinafine represents one of the more affordable prescription treatments even without insurance coverage.
What blood tests will I need before and during treatment?
Both medications require baseline liver function testing before treatment initiation, including ALT, AST, alkaline phosphatase, and bilirubin measurements. Complete blood count testing is recommended for patients with known hematological conditions or immune system concerns. For Lamisil, follow-up liver function testing typically occurs at 6 weeks for standard 12-week treatment courses. Patients with baseline abnormalities or risk factors may require more frequent monitoring. Sporanox typically requires more intensive monitoring, with liver function tests recommended monthly during continuous therapy. Additional cardiac evaluation including ECG may be recommended before Sporanox treatment for patients with cardiac risk factors or those taking medications that might interact with itraconazole.
Can I use these medications if I’m pregnant or breastfeeding?
Neither medication is recommended during pregnancy. Lamisil is classified as FDA Pregnancy Category B, indicating no evidence of risk in animal studies but insufficient human data to confirm safety. Sporanox carries greater concerns as a Category C medication, with animal studies showing potential embryotoxicity at high doses. Due to the non-urgent nature of fungal nail infections, postponing treatment until after pregnancy represents the safest approach.
For breastfeeding mothers, Lamisil is excreted in breast milk and not recommended during nursing. Limited data exists on Sporanox in breast milk, but manufacturers recommend against use during breastfeeding due to theoretical risks. Given the cosmetic nature of most nail fungus treatments, delaying therapy until after weaning represents the most conservative approach. For severe infections requiring immediate treatment, temporary cessation of breastfeeding with pumping and discarding milk during treatment might be considered in consultation with your healthcare provider. For more information on severe toenail fungus treatment, consult with a specialist.
If you’re planning pregnancy in the near future, completing treatment at least one month before conception attempts is generally recommended for both medications.